Hey guys. This time I’m going to post about something that is a bit more complex but very interesting part of our body. In my opinion, Neuroanatomy is one of the more difficult subjects to digest as compared to other body parts because the structures are smaller and refined yet very important. Acquiring proper knowledge on how this part of the brain works is essential in diagnosing certain diseases especially when the world nowadays is populated with many diabetic patients. These patients are prone to get nerve damage in the form of diabetic neuropathy. Today I’m going to describe about the Cranial Nerves which relays information between the brain and the other parts of the human anatomy, especially in the head and neck region.
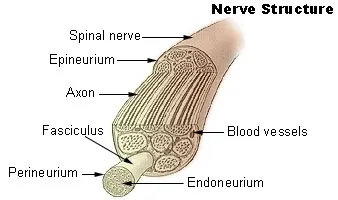
Before I explain about the cranial nerves, let us understand the basic anatomy of a nerve. The nervous system is made up of two different cells, namely Nerve cells or neurons, and Glial cells. Nerve cells are the most basic functioning unit of any nerve and Glial cells on the other hand, provide support to the nerve cells.
The structure of neuron cells are divided into four:
- Cell body
- Dendrites
- Axons
- Axons Terminal
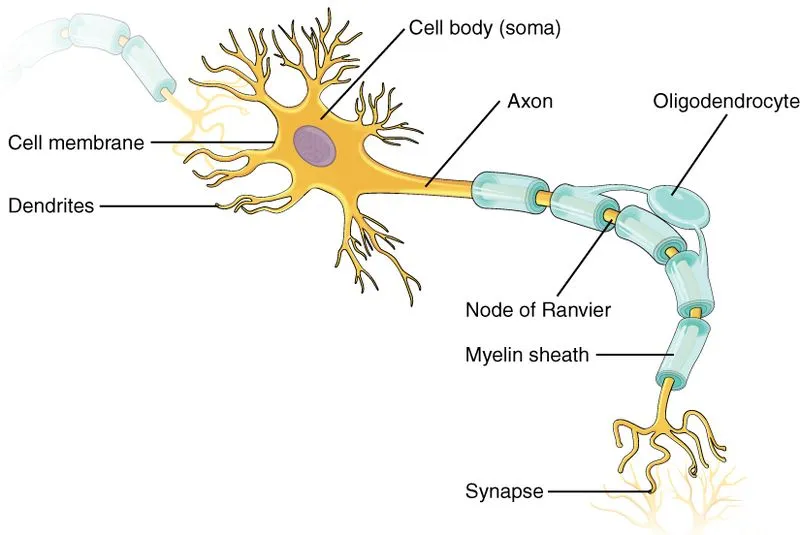
The cell body contains the nucleus and similar to other type of cells, nucleus is the main intelligence unit of the cells. Dendrites are the elongated portions of the nerve cells and their function is to receive signals from other cells. Axons are long, thin structures where the nerve impulse moves. A normal nerve cell could have multiple dendrites but just only one axon. Each axons are covered with myelin sheath. Myelin sheath is an insulating layer that protects the axon.
In between each myelin sheath, there’s a gap. The gap is known as the Nodes of Ranvier .They allow saltatory conduction of nerve impulses, in which they help to increase the conduction velocity of action potentials. Basically, they speed up the nerve conduction process. Axons terminal are the most distal part of an axon, from here they transmit signals to other nerve cells.
To enhance the transmission, the terminals contain a huge number of mitochondria. These mitochondrias produces energy in the form of ATP (Adenosine TriPhosphate). Many other cells contain mitochondria as these are the factories to produce energy to the cells.
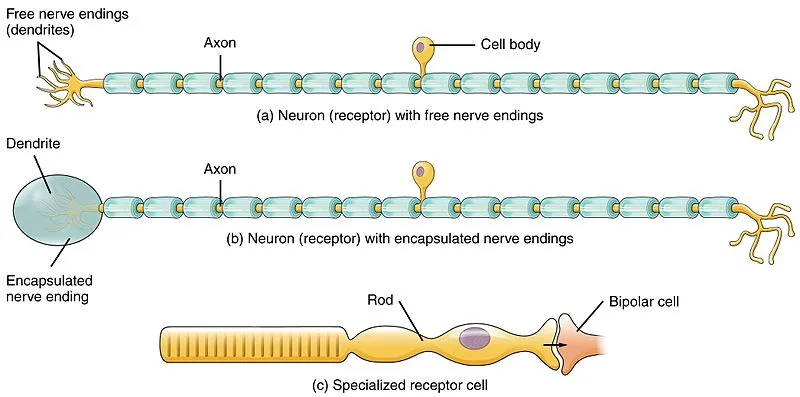
After understanding the basic anatomy of the nerve cell, let’s talk about the functions. Nerve cells are categorized according to their functionality, namely the sensory nerves, motor nerves and intermediate nerves. Sensory nerves as the name implies, receives sensation. It depends on the type of sensory organ that you are talking about. For example, the sensory nerves in the eye receives light, the sensory nerves embedded in the skin receives touch stimulation and those in the nose receives odour. Sensory nerves are often the afferent neurons as they receive impulses from the environment. Motor nerves are the efferent neurons as they conduct impulses from the higher centers towards the parts that they supply. Some of these efferent neuron innervates the muscles to allow movements, and as the name implies, motor.
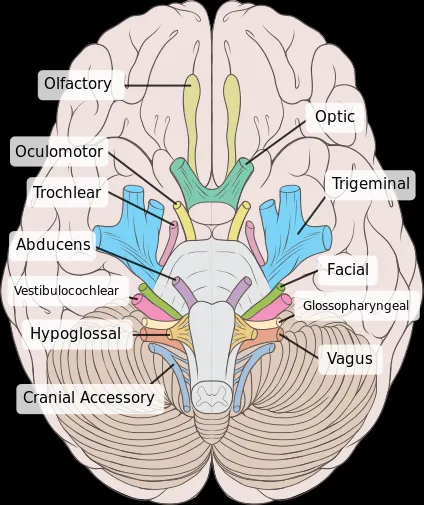
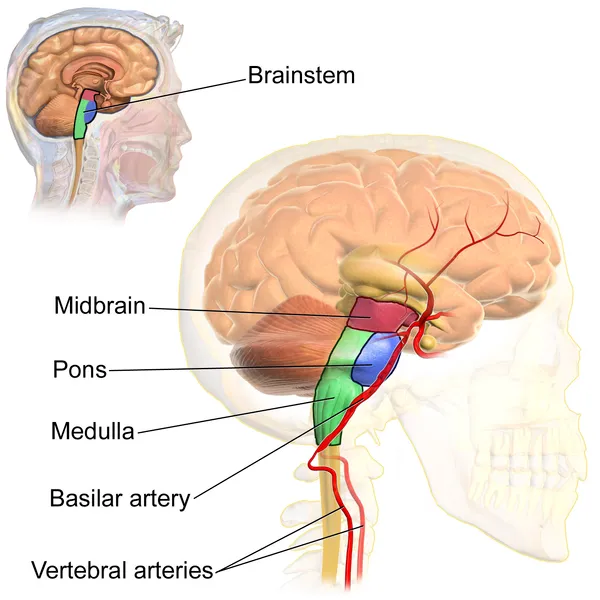
Let’s talk about the main bulk of this topic, which are the cranial nerves. I’m going to go based on their anatomical location, their importance and finally what diseases are related to each nerves. There are 12 pairs of cranial nerves that arise from the brain. The first two cranial nerves came from the cerebrum or the forebrain and the remaining 10 nerves originate from the brainstem. The brainstem is divided into midbrain, pons and medulla hence the 10 latter nerves either came from each of the three parts or from the junctions of each part.
Cerebrum – Olfactory (CNI) and Optic (CNII)
Midbrain – Trochlear (CNIV)
Midbrain-Pontine Junction – Oculomotor (CNIII)
Pons – Trigeminal (CNV)
Pontine-Medulla Junction – Abducens (CN VI), Facial (CNVII) and Vestibulocochlear (CNVIII)
Medulla Oblongata – Glossopharyngeal (CNIX), Vagus (CNX), Accessory (CNXI), Hypoglossal (CNXII)
CN1 – Olfactory Nerve
Olfactory nerve is the shortest cranial nerve. The nerve is purely sensation as they transmit the sensory of smell from the nose. They have the capability to regenerate and it is unmyelinated. When a specific odour enters the nose, the receptors which are located in the olfactory mucosa of the upper parts of nasal cavity are then stimulated. The nerves enter the cranial cavity and to the olfactory bulb. The sensation is then passed to the olfactory tract. The olfactory extends to the many parts of the brain including the piriform cortex, the amygdala, olfactory tubercle and the secondary olfactory cortex. These parts are quite complex but to simplify, these regions involve in the memory and appreciation of odours.
Clinical Relevance
Anosmia. It is defined as the absence sensation of smell. Temporary anosmia is common in common colds or any traumatic injury of the nose. A permanent anosmia, which is more important, can be caused by head injuries, or tumours. Neurodegenerative disorders such as Parkinson’s or Alzheimer’s can result in Anosmia but the symptoms are much more insidious compared to the causes I have mentioned above.
CNII – Optic Nerve
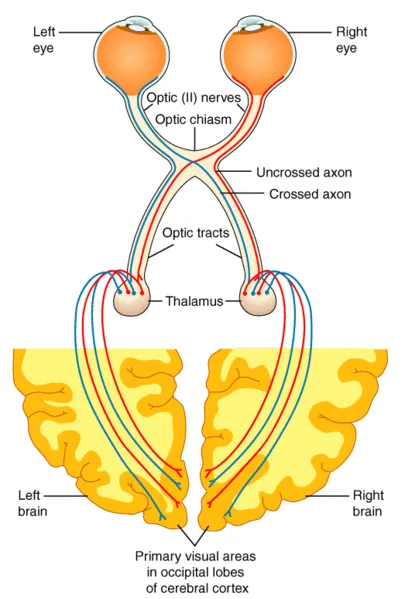
As the name implies, it is capable of transmitting the light sensation. They receive impulses from the photoreceptors of the eye (rods and cones) and leaves the eye through the optic canal, which is a pathway on the sphenoid bone. After passing through the sphenoid bone, they unite with the other optic nerve from the other eye to form the optic chiasm. Half of the nasal fibres cross over and forms the optic tract. Each optic tract then reaches the Lateral Geniculate Body and then to the optic radiation. The optic radiation is connected to the visual cortex, which is a part of the brain that processes the light stimulus and this area responds appropriately. The visual pathway is quite complex but it is understandable. I suggest you guys to read up more about the types of vision problems that can happen based on the disruption of each anatomical part of the visual pathway.
Clinical Relevance
Pituitary Adenoma, which is a tumour in the Pituitary Gland, can cause compression to the Optic Chiasm due to the close proximity between those two structures. The individual might be experiencing a vision called the Tunnel Vision due to the compression of the Optic Chiasm.
CN III – Oculomotor Nerve
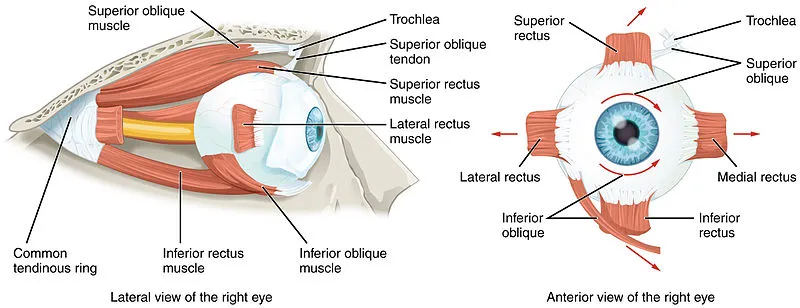
This nerve provides motor innervation to most of the eye muscles as well to the sphincter pupillae, which involves in pupil constriction. It originates from the midbrain and passes below the posterior cerebral artery and leaves the cranial cavity via the superior orbital fissure. After that it divides into the superior and inferior branches. The superior branch supplies the superior rectus (one of the muscles that controls the eye movement) and the levator palpabrae superioris (a muscle that raise the eyelid). The inferior branch supplies the other eye muscles and also the sphincter pupillae.
Clinical Relevance

Oculomotor nerve lesions can be caused by brain tumours, aneurysm of the posterior cerebral artery or a much more common condition which is long standing Diabetes Mellitus. Diabetes is a well-known condition to cause nerve damage, which is known as neuropathy. Since the levator palpabrae muscle is affected, the individual might have ptosis(drooping of eyelid) of the particular eye . The pupil of that eye might be dilated despite being shined by a torchlight because of the sphincter pupillae’s muscle impairment. I received this case during my shortcase examination when I was a third year medical student. Before the exam, I’ve never encountered any patients with Cranial Nerve III palsy but thanks to this theory part which I have read before, I’ve managed to get the diagnosis right. Hehe.
CN IV – Trochlear Nerve
This is the smallest and yet the longest nerve! It’s purely motor as it supplies the superior oblique muscle of the eye. This nerve originates from the midbrain and moves along the cavernous sinus before piercing to the eye via the superior orbital fissure. Remember SO4 and LR6 - Superior oblique muscle is supplied by the CNIV and the lateral rectus muscle is supplied by the CNVI
Clinical Relevance
If the nerve is damaged, the function of the superior oblique muscle is impaired too. The function of this muscle is to assist the eye in looking downwards and inwards, thus the individual will experience diplopia (double vision) if we ask him/her to look downwards and inwards.
CNV – Trigeminal Nerve
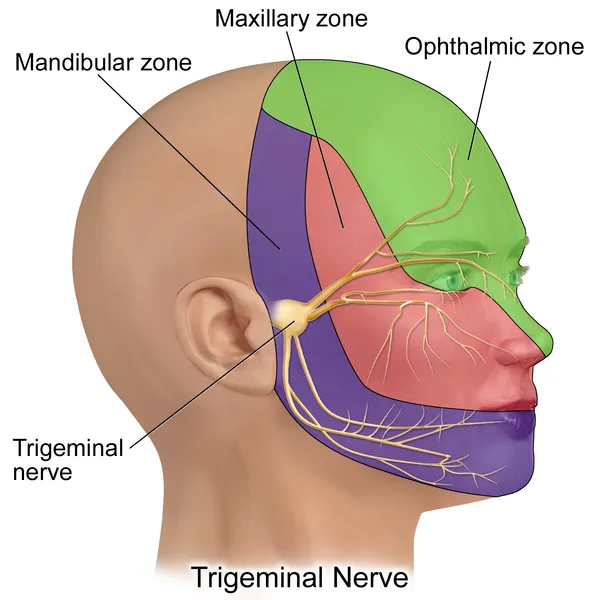
It is the largest cranial nerve and it has both sensory and motor innervation. For the sensory part, it has three branches mainly supplies the sensation of the face. The motor part supplies the muscles of mastication (or chewing). They arise from the pons and enters the middle cranial fossa. Here, the sensory root divides into three branches, namely the Opthalmic, Maxillary and Mandibular. Hence, that's the reason why they call it TRIgeminal which indicates its three distinct branches. The motor nerves passes below the sensory root and towards the Mandibular division as this division supplies the muscles of chewing. The ophthalmic branch exits the cranium via the superior orbital fissure and the Maxillary branch exits via the foramen rotundum. The mandibular nerve exits via the foramen ovale.
- Opthalmic branch supplies the forehead, scalp, upper eyelid, conjunctiva, cornea, dorsum aspect of the nose and the lacrimal gland.
- Maxillary branch supplies the lower eyelid, conjunctiva, cheeks, nasal cavity, lateral nose, upper lip, upper teeth, superior palate and both the lacrimal and nasal glands.
- The sensory Mandibular branch supplies the floor of mouth, external ear, lower lip, chin, anterior 2/3 of the tongue, lower teeth. The motor Mandibular branch supplies the muscles of chewing, suprahyoid muscles, and some muscles of the ear.
Clinical Relevance
Individuals with Trigeminal nerve problems might have loss of corneal reflex as well because the ophthalmic branch of the trigeminal nerve is involved in this reflex, alongside the facial nerve. Some of the muscles of the ear are supplied by this nerve as well. As an example, the tensor tympani muscle which functions to dampen sounds might have the dampening ability impaired. Hence, the individual might complain of hyperacusis (increase in sensitivity to certain volume frequency).
CNVI – Abducens Nerve
This nerve has purely motor innervation. It innervates the lateral rectus muscle of the eyeball. This nerve originates from the junction of pons and medulla and travels through the cavernous sinus at the tip of petrous temporal bone. After that it exists the cranium via the superior orbital fissure and innervates the lateral rectus muscle.
Clinical Relevance
Conditions such as brain tumour and diabetes mellitus can cause impairment to this nerve’s function. Individuals with this nerve problem can complain of diplopia and a medially rotated eye. The function of lateral rectus is to move the eyeball “laterally”, thus if there’s any problem with this muscle, the eye will tend to move medially.
For me, cranial nerves are intriguing as they are the main transportation means of our sight, smell, and hearing from the sensory organs to the brain. Alright. That's all for this part. I'll continue the second part which will cover on the other Cranial Nerves (CNVII to CNXII) in the next post.
References
- The Cranial Nerves. Teach Me Anatomy. Retrieved on April 8, 2018, from http://teachmeanatomy.info/head/cranial-nerves/
- Ultrastructure of Nerves. Teach Me Anatomy. Retrieved on April 8, 2018, from http://teachmeanatomy.info/the-basics/ultrastructure/nerves/
- Cranial Nerve Examination. Geeky Medics. Retrieved on April 8, 2018, from https://geekymedics.com/cranial-nerve-exam/#2
- Cranial Nerves. Wikipedia. Retrieved on April 8, 2018, from https://en.wikipedia.org/wiki/Cranial_nerves