
My research over the past two years has led me to suspect that there is no such disease as COVID-19. This is the opinion of many doctors and epidemiologists, who have been critical of the official narrative:
Mark Bailey & John Bevan-Smith:
COVID-19 is a fraud because its alleged causal agent, a purported novel coronavirus called SARS-CoV-2, has not been proven to exist in nature and therefore has not been established as the cause of COVID-19, the disease and pandemic invented by the World Health Organization ... the misapplication of the PCR means that COVID-19 is a scientifically meaningless construct that represents nothing more than a referential illusion ... The COVID-19 fraud is the work of international elites, the pharmaceutical industry, and complicit politicians working to a globalist agenda, the purpose of which appears to be the extinguishing of human rights and freedoms and the dismantling of democracy for purposes of controlling populations and the extortion of vast sums of money from countries on the basis that a disease, COVID-19, invented by the WHO, poses a serious threat to their populations. (Bailey & Bevan-Smith 3 ... 23 ... 33)
Samantha Bailey:
One of the first documented clusters of what has been deemed COVID-19 was in December 2019 in Wuhan, China when 41 patients with pneumonia were hospitalised. The most common symptoms were fever (98%), cough (76%), and myalgia or fatigue (44%). Abnormalities were reported in chest CT images for all patients as would be expected for a diagnosis of pneumonia. Six of the patients died. There were no specific symptoms or general laboratory findings that would allow for classification of a new type of respiratory illness or for a novel pathogen to be implicated as the monocausal agent. (Bailey)

But many other doctors who are equally suspicious of the official narrative insist, nevertheless, that COVID-19 is a real disease or disorder. Perhaps it is not caused by a virus, or perhaps it is not nearly as serious as the World Health Organization says it is, but people are falling ill with a dangerous respiratory sickness that can be clearly distinguished from known respiratory illnesses and disorders, such as influenza, pneumonia, tuberculosis, bronchitis, bronchiolitis, asthma, the common cold, allergies, etc.
Tom Cowan:
In the case of “COVID,” I have no objection to exploring the hypothesis that some infectious agent is the cause of this potentially new illness, but I also contend that many other possible causes should be explored ... For me, “COVID” is many things, but, fundamentally, it is a crisis of how we see biology; that is, how we view life. (Cowan 2-3 ... 31)
Sebastian Rushworth:
I am not denying that covid is awful for the people who do get really sick or for the families of the people who die, just as it is awful for the families of people who die of cancer, or influenza, or an opioid overdose. But the size of the response in most of the world (not including Sweden) has been totally disproportionate to the size of the threat. (Rushworth)
Peter A McCullough:
Acute COVID-19 has a great range of clinical severity from asymptomatic to fatal. In the absence of clinical trials and guidelines, with hospitalizations and mortality mounting, it is prudent to deploy treatment for COVID-19 based on pathophysiological principles. We have proposed an algorithm based on age and comorbidities that allows for a large proportion to be monitored and treated at home during self-isolation with the aim of reducing the risks of hospitalization and death. (McCullough)

In this article I am examining the possibility that at least some alleged cases of COVID-19 are psychosomatic.
Psychosomatic Symptoms
Somatic symptom disorder is a well-attested mental disorder in which a patient presents with physical symptoms consistent with illness or injury but for which no physical cause can be detected. Although this disorder is said to have been first formally described in 1859 by the French psychologist Paul Briquet, one form of the disorder—hypochondria—has been known for centuries. The Oxford English Dictionary traces this particular use of the term to 1668:
Hypochondria ... 2. as sing. A morbid state of mind, characterized by general depression, melancholy, or low spirits, for which there is no real cause ...
1668 Dryden Even. Love [An Evening’s Love] iv. ii, I know what you would say, that it is melancholy; a tincture of the hypochondria you mean. (OED 5:507-508)
In Molière’s comedy Le Malade imaginaire of 1673, a hypochondriac betroths his daughter Angélique to a physician so that he will have constant access to the doctor’s services. At the end of the play, he allows Angélique to marry her lover Cléante only on condition that Cléante become a doctor.

In 1798, Immanuel Kant discussed hypochondria in Anthropology from a Pragmatic Point of View:
The hypochondriac’s illness consists in this: that certain internal physical sensations are not so much symptoms of a real disease present in the body as rather mere causes of anxiety about it; and that human nature has the peculiar characteristic (not found in animals) that paying attention to certain local impressions makes us feel them more intensely or persistently—on the other hand, when our attention is turned away from them either deliberately or by other distracting occupations, they subside and, if our abstraction becomes habitual, stop completely. This is how hypochondria, as morbid anxiety, causes the patient to imagine that he is physically ill: though he knows that the illness is a product of his imagination, now and then he cannot help taking the image for something real or, vice-versa, making out of a real physical complaint (such as the discomfort that follows a meal of flatulent food) images of all sorts of serious external events and worries about his business, which vanish as soon as he has finished digesting his meal and the flatulence stops. (Kant & Gregor 82-83)
Molière and Kant were describing people who imagined they were suffering from all sorts of ailments but who were, in fact, in perfect health. It is now acknowledged by the medical profession, however, that patients may present with very real, physical symptoms whose causes are entirely psychological.
The Nocebo Effect
Most of us a familiar with the Placebo Effect: the tendency of any medication or treatment, even an inert or ineffective one, to exhibit results simply because the recipient believes that it will work.
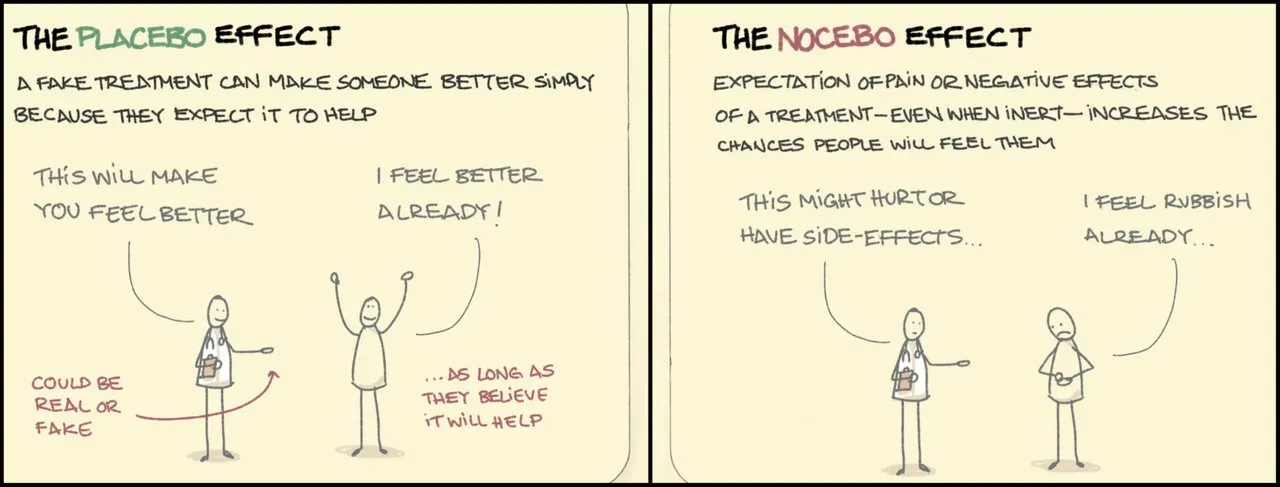
Less well-known is the Nocebo Effect: a patient’s negative expectations regarding a treatment cause the treatment to have a more negative effect than it would otherwise have. It is not unknown for a patient to suffer a side-effect of a particular medication in cases where they actually received an inert placebo.
These effects are believed to be psychogenic. That is to say, they have psychological rather than physiological causes. Underlying both is the power of suggestion. An article published ten years ago by HealthDay, the World’s largest syndicator of health news, summed up the Nocebo Effect with the phrase: If You Think You’ll Get Sick, You Will:
The ‛Nocebo’ Effect: If You Think You’ll Get Sick, You Will
Study author suggests doctors give patients less info on potential drug side effects, but is that ethical?
Some patients will feel better after taking a medication even if the drug doesn’t actually do anything to treat their condition. It’s called the “placebo effect.” But there’s another side to the power of suggestion: Patients may develop symptoms and side effects purely because they’ve been told about them. A new report analyzes the so-called “nocebo effect” and suggests that doctors learn how to better “exploit the power of words” for the benefit of patients. (Dotinga)

Munchausen Syndrome by Proxy
The Nocebo Effect may be psychogenic, but the disorder whose treatment triggered the effect may be a real one, with genuine, clinical symptoms. There are, however, psychosomatic disorders in which the disease itself is created by the power of suggestion. Of these, Munchausen Syndrome by Proxy is considered a rather extreme example. It is defined as a factitious disorder imposed on another—a condition in which a caregiver creates the appearance of health problems in another person. The illness is factitious—made up—and the caregiver acts consciously and intentionally. Nevertheless, the victim may exhibit very real symptoms and doctors may be fooled into prescribing unnecessary or ineffective treatments.
Munchausen’s Syndrome was first named and described by the English endocrinologist Richard Asher in 1951 as a mental disorder in which an individual creates a factitious disease—inventing or exaggerating clinical symptoms—to gain attention or sympathy for themselves. Munchausen Syndrome by Proxy was first used in a 1976 paper by John Money and June Faith Werlwas to describe a related mental disorder in which the instigator of the factitious disease is not the alleged sufferer but another person—typically the victim’s carer.
Could COVID-19 be a sort of Munchausen Syndrome by Proxy? It certainly cannot be denied that bodies charged with the health and well-being of the global population—the CDC, the WHO, the Johns Hopkins University School of Medicine, governments, etc—have been among the most vociferous spreaders of fear in relation to covid. They have consistently endorsed apocalyptic models of the pandemic, such as Neil Ferguson’s wildly inaccurate predictions, while silencing dissenting voices calling for a calm and measured response to any health emergency.
Covid-19
For the better part of two years—2020-2022—the entire population of the World has been subjected to a continuous barrage of covid-induced paranoia. Newsfeeds have been regurgitating an endless stream of fear porn. Governments and mainstream media outlets have been unremitting in their attempts to spread panic among the populace. The gaslighting of entire nations has been relentless. In the light of such an unprecedented campaign to convince the global population that the planet is in the grip of one of the worst pandemics in human history, is it any wonder that millions of people worldwide have presented in emergency rooms with symptoms of the very disease they were warned of? How many of these “cases” were psychosomatic?
How many people are suggestible to such a degree that they can develop symptoms of a disease that is entirely factitious. In 1943, the renowned psychologist Hans Jürgen Eysenck estimated that two-thirds of men and one-third of women are suggestible:
These figures show that roughly two-thirds of the men are suggestible, while only one-third of the women are suggestible according to our criterion. This difference is definitely statistically significant and shows that ... women tend to be less suggestible than men. (Eysenck 350)
Assuming that there are approximately as many men as women in the World, this means that 50% of the global population are suggestible. Eysenck found that psychological disorders were not relevant: subjects suffering from neuroses or hysteria were neither more nor less suggestible than “well-adjusted” subjects (Eysenck 349-350).
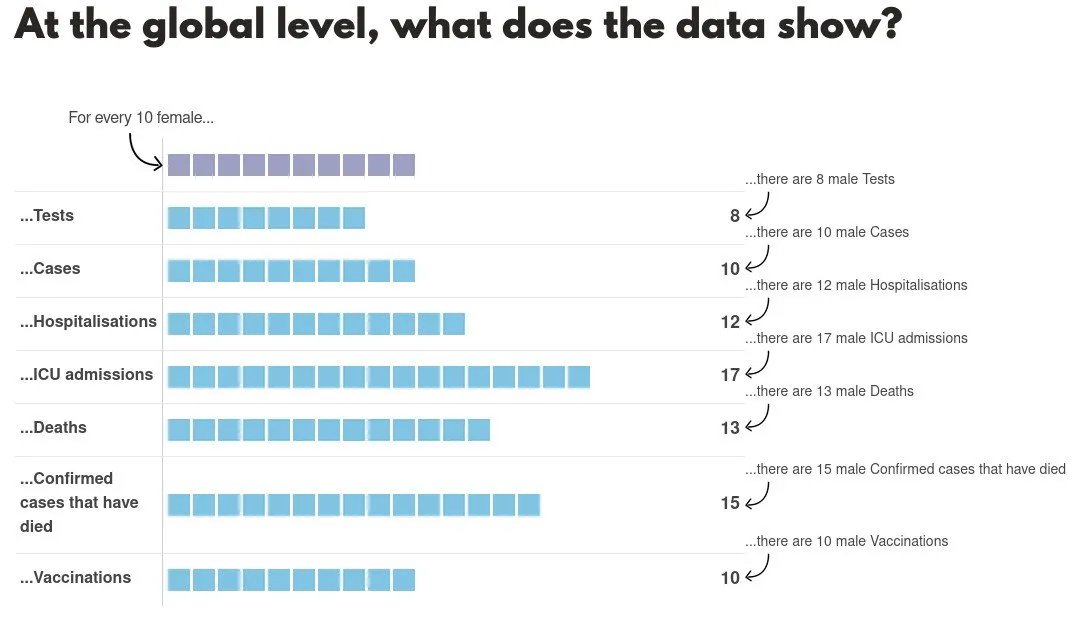
It is interesting to note that according to the The Sex, Gender and COVID-19 Project, of the 6.2 million people who are said to have died of COVID-19, 56% were male and 43% female. For “confirmed cases”, the figures are 60% and 40% respectively. Epidemiologists have been at a loss to explain this disparity. According to an article published in The New York Times in January 2022, “It’s Complicated”:
Early on, some scientists suspected the reason was primarily biological ... But a new study analyzing sex differences in Covid-19 deaths over time in the United States suggests that the picture is much more complicated.
While men overall died at a higher rate than women, the trends varied widely over time and by state, the study found. That suggests that social factors—like job types, behavioral patterns and underlying health issues—played a big role in the apparent sex differences, researchers said.
“There is no single story to tell about sex disparities during this pandemic, even within the United States,” said Sarah Richardson, director of the GenderSci Lab at Harvard University, which studies how biological sex interacts with cultural influences in society ...
Sex differences in genes, hormones or immune responses are not likely to explain these differences, the researchers said.
“There would be no reason for biology to be that variable across time and space,” said Katharine Lee, a biological anthropologist and engineer at Washington University in St. Louis and an author of the new study. (Ghorayshi)
Other theories that have been postulated to explain the disparity include:
Women’s immune systems are stronger than men’s.
Men tend to engage in riskier behaviour, such as ignoring physical distancing or not wearing masks.
Men don’t take symptoms as seriously as women do, and are less likely to seek medical help.
No one else seems to have raised the possibility that at least some of the alleged cases of COVID-19 are psychosomatic. Sex disparity in the suggestibility of humans may be a crucial factor in explaining the sex disparity observed in the “covid” death toll.
COVID-19 Testing and Misdiagnosis
If some cases of COVID-19 were psychosomatic, then it is possible that a number of perfectly healthy individuals developed a factitious disease that then killed them. But even if we consider this an unlikely occurrence, there remains the possibility that a significant number of people developed a genuine respiratory illness—the common cold, influenza, pneumonia, bronchitis, etc—which was then fatally exacerbated by their belief that they were suffering from the deadly COVID-19. In the early stages of the pandemic, health officials even warned the public of the danger of “false negatives” in COVID-19 testing, advising symptomatic people to assume that they had the disease even if their test came back negative (Healthline, 13 April 2020).
During the pandemic, people who presented at hospital with one of these common respiratory illnesses were routinely given a PCR test. Many of these people tested positive. They were then informed by a doctor that they had COVID-19, and they believed it—whether they were suggestible or not. How many of these people died from the flu, pneumonia, or even a common cold because they and their doctors believed they had COVID-19? How many died because they unconsciously aggravated their symptoms to the point where they became fatal? How many died because they were treated for a disease they did not have, while the disease they did have went untreated?
The misuse of PCR during the pandemic is too serious a subject to be dealt with in a few paragraphs tacked on to the end of this article. We will, therefore, devote the whole of the next article to that particular rabbit-hole.
And that’s a good place to stop.
References
- Mark Bailey & John Bevan-Smith, The COVID-19 Fraud & War on Humanity, Online (2021)
- Samantha Bailey, What is “COVID-19” and Where Is the “Pandemic”? Online (2021)
- Tom Cowan, Breaking the Spell: The Scientific Evidence for Ending the Covid Delusion, Tom Cowan (2021)
- Randy Dotinga, The ‛Nocebo’ Effect: If You Think You’ll Get Sick, You Will, HealthDay News, Online (2012)
- Hans Jürgen Eysenck](https://journals.sagepub.com/doi/pdf/10.1177/003591574303600713), Suggestibility and Hypnosis—An Experimental Analysis, Proceedings of the Royal Society of Medicine, Volume 36, Issue 7, Pages 349-354, Royal Society of Medicine, London (1943)
- Immanuel Kant & Mary J Gregor (translator), Anthropology from a Pragmatic Point of View, Martinus Nijhoff, The Hague (1974)
- Molière & Henri van Laun (translator), Le Malade imaginaire [The Imaginary Invalid], The Dramatic Works of Molière, Volume 3, Gebbie & Barrie, Philadelphia (1879)
Image Credits
- COVID-19 Poster: © 2021 Dublin Region Homeless Executive, Fair Use
- Samantha Bailey: © Idealog, Fair Use
- Tom Cowan: © Dr Tom Cowan, Fair Use
- Le Malade imaginaire: Honoré Daumier (artist), Philadelphia Museum of Art, Public Domain
- The Placebo Effect and the Nocebo Effect: © Sketchplanator, Fair Use
- Munchausen Syndrome by Proxy: © Osmosis, Creative Commons License
- Covid-Related Sex Disparity: © Global Health 5050, Creative Commons License
- If You Have Symptoms, Assume You Have the Disease: © Getty Images, Fair Use
Video Credits
- How Coronavirus Fear Porn Will Make You Sick : © David Seaman, Fair Use
Online Resources
- What Is Covid-19 and Where Is the Pandemic?
- RIP.ie
- Central Statistics Office (CSO)
- Northern Ireland Statistics and Research Agency (NISRA)
- EUROMOMO
- Our World in Data
- Rational Ground
