ESSAY
The Growing Trend of Violence Committed By Patient Relatives Against Medical Professionals
BY
CIVIL ENGINEER AWAIS KHAN
UET PESHAWAR
+923219884792
- INTRODUCTION
- DEFINITION OF VIOLENCE
- SURVEYS CONDUCTED IN HOSPITALS
- CAUSES OF VIOLENCE
4.1. COMMERCIALIZATION AND CORRUPTION
4.2. ROLE OF MEDIA
4.3. VULNERABLE AREAS
4.4. OTHER CAUSES IN ED
4.5. COMMUNICATION
4.6. SECURITY
4.7. JUDICIAL SYSTEM
4.8. FEMALE WORKERS
4.9. REGION SPECIFIC CAUSES - SOLUTIONS TO MITIGATE VIOLENCE
5.1. RAISING STANDARDS
5.2. MUSHROOM GROWTH
5.3. QUANTITY AND QUALITY
5.4. FALSE HOPE
5.5. AVOIDING NEGLIGENCE
5.6. EXPERIENCED PROFESSIONAL ADMINISTRATORS
5.7. EFFICIENT SYSTEM
5.8. CONFIDENCE BUILDING
5.9. PERIODIC UPDATES
5.10. PUBLIC RELATIONS
5.11. PEMRA’S ROLE
5.12. SECURITY
5.13. BEST STAFF
5.14. CONSULTATION
5.15. AWARENESS
5.16. ONE GUEST POLICY
5.17. NO SYNDICATES POLICY
5.18. HELP FROM TECHNOLOGY
5.19. PROTECTION FOR AMBULANCES
5.20. HOTLINE
5.21. RAPID RESPONSE TEAM
5.22. INCREASED BUDGET
5.23. STRICT VISITING HOURS
5.24. IDENTIFICATION
5.25. COMPLAINT CELL
5.26. MEDICAL COST
5.27. BLACK MARKET - CONCLUSION
- REFERENCES
INTRODUCTION: Larkana: A 25-years old patient named Tasneem wife of Abdullah Leghari, a resident of Miro Khan Taluka of Kambar-Shahdadkot district, a resident of OPF Colony of Larkana was rushed to hospital in critical condition and the duty doctors suspected that she had tried to commit suicide.Her stomach was washed immediately but she could not survive.The attendants of the patient called their relatives. The relatives around arrival ransacked office of Chief CMO, broke office furniture, windowpanes, fired pistol shots and severely beat duty doctors at Accident & Emergency Center of the Chandka Medical College Hospital, as they suspected that their patient died due to the negligence of duty doctors. They tore clothes of one Dr. Mannan Bhutto and dragged him in the emergency ward. Zahid Leghari, a relative of the patients, told media that she died due to the negligence of duty doctors. Chief RMO Dr. Habib Soomro said that the accused also fired straight pistol shots but fortunately no one was injured as all the doctors and duty staff had already fled. Police arrived one hour late despite informing them well on time and they played a role of silent spectator and not arrested a single accused. Assistant Commissioner Masood Bhutto and DSP Yar Muhammad Rind later held talks with the enraged people and the situation was brought under control. The Medical Superintendent of Chandka Hospital has constituted a 3-member probing committee consisting of Prof: (Rtd.) Hafeezullah Abro, I/C Accident & Emergency Center, Dr. Abdul Majeed Jessar and Dr. Ahmed Ali Brohi, both Additional Medical Superintendents of the Hospital to report within three days. No case was filed till filing of this report [1].
The purpose of citing the above story is not to show an event of violence that took place in a rural area of Pakistan rather it was meant to show that incidents like that have become a norm in almost all medical institutes of Pakistan; varying in intensity and damage inflicted. The reasons for violence inflicted against clinicians are many and varied. Violence is a function of the dynamic interaction between a specific individual and a specific situation for a given period. Patients who feel they have been physically and/or psychologically injured are at increased risk for committing violence against clinicians, especially if their complaints are dismissed. Fear and helplessness are risk factors for patient violence, especially when painful intrusive procedures are used.DEFINITION OF VIOLENCE: The World Health Organization (WHO) defines violence as ‘’ the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, which either results in or has a high likelihood of resulting in injury, death, psychological harm, underdevelopment or deprivation.”[2]
SURVEYS CONDUCTED IN HOSPITALS: Pakistani society is currently passing through political turmoil and political instability. Poverty, unemployment, and political agitation have generated frustration, anger, and impatience among mango people resulting in a spike in crime and violence trend in the country. Among many communities, the medical community is also being immensely targeted by this crime and violence. A study carried out in 2011 shows that nearly 77% of 675 doctors from 9 public hospitals in Pakistan had experienced violence — 65 percent verbal and 11.9 percent physical. [3] In another similar study in 2013, conducted on 164 healthcare professionals from a public health care facility in Lahore, 74% of the doctors admitted that they experienced violence while working in the emergency department. The offenders were mostly patients' relatives 71%. [4]. Both the reports concluded that "too many" attendants, long waits, limited contact with the physician, resulted in chaos and mayhem and in turn, led to violent incidents.
CAUSES OF GROWING TREND OF VIOLENCE PERPETRATED BY PATIENT RELATIVES IN HEALTH-CARE SETTINGS:
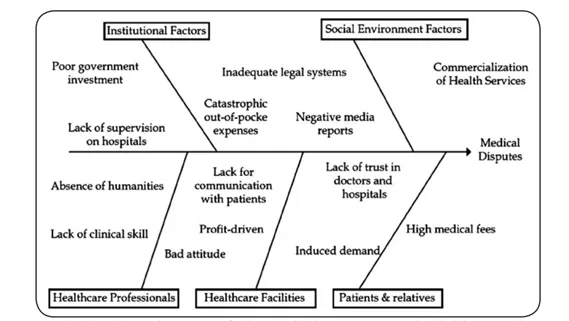
Figure 1: Causes
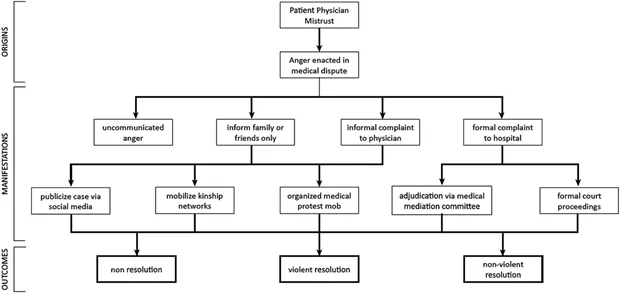
Figure 2: Schematic of pathways from patient-physician mistrust to outcomes of medical disputes.
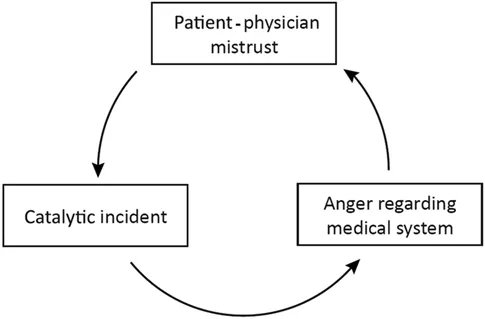
Figure 3: Vicious Cycle of Unintended Consequences Resulting From Mistrust And Medical Disputes.
4.1. COMMERCIALIZATION AND CORRUPTION: Surge in the commercialization of medical profession coupled with widespread corrupt unethical practices by the medical professionals lead to the increase in violence against healthcare professionals.
4.2. ROLE OF MEDIA: the Negative role of media in portraying a villainous image of medical institutes and professionals working in them has stirred the emotions of mistrust and hatred among the masses.
4.3. VULNERABLE AREAS: Emergency wards/departments are the most vulnerable places to the threat of violence. The sources of violence are Patient’s relatives; brainwashed by negative media reports; irritated by personal socio-economical deprivations; agitated by an inhumane irritating attitude of the staff.
4.4. OTHER CAUSES IN ED: The other causes that can trigger violence in Emergency Departments include i. Patient and relatives’ assumption that they are not provided proper treatment by the staff.
ii. Fatality of patients can bring out the worst behavior in the relatives even though appropriate treatment might have been given in serious cases.
4.5. COMMUNICATION: Lack of communication between Doctor and patients due to the difference in language, social status, gender difference can also become a cause of ferocity.
4.6. SECURITY: Insufficient security for medical staff makes them an easy target for an angry mob of relatives.
4.7. JUDICIAL SYSTEM: An Incompetent judicial system that cannot provide justice; take away the fear of rule of law and thus make it easier for the people to take the law into their hands and inflict damage upon anyone they desire.
4.8. FEMALE WORKERS: Lady Health workers (Nurses) are more vulnerable to violent incidents as compared to their male counterparts. The reasons for this violent behavior are usually excessive waiting time, shortage of staff and unmet patients demands. Verbal abuse was the most common and the assailants were mostly the patient's relatives or friends followed by the patients themselves.[5]
4.9. REGION SPECIFIC CAUSES: Whilst most of the causes that can trigger violence are common in many Asian countries, some may be specific to certain countries. For example in China, the authors report little incentives to the hospital directors to improve the quality of service, inefficient supervision besides problems in medical education like deficiencies in curriculum, absence of humanistic education, traditional teacher-centered teaching methods, mushroom growth of medical schools which now number 644 that includes 146 institutions for higher education for medicine and 498 secondary vocational schools.(Chinese Education Statistical Year book 2012) This has resulted in a six-fold increase in annual enrolment from 75,000 in 1998 to almost 450,000 in 2008.[6] A similar situation is witnessed in countries like India, Pakistan, and Bangladesh where there is the mushroom growth of private medical and dental schools during the last couple of years with the result that the number of medical and dental institutions in private sector are much more as compared to the public sector in all these three countries. Many of these institutions do not have enough teaching and training facilities, their own affiliated teaching hospitals hence it has certainly affected the quality of training.
All this shows how widespread this violence against the healthcare professionals has become. The situation is so worse that some even suggest to let the healthcare professionals should be allowed to carry weapons along with their selves or learn some physical sports like Judo, Karate etc. in order to protect themselves.
- SOLUTION TO TACKLE CAUSES OF GROWING TREND OF VIOLENCE PERPETRATED BY PATIENT RELATIVES IN HEALTH-CARE SETTINGS
As such it is high time that authorities in these countries wake up and initiate some effective measures. Some of these could be as under:
5.1. RAISING STANDARDS: Accreditation criteria for medical and dental schools should be made very strict in order to maintain high quality and standards. Those institutes failing to raise their standard to the prescribed criteria should be closed down.
5.2. MUSHROOM GROWTH: The Mushroom growth of medical and dental schools should be monitored strictly and new institutes allowed to work should fulfill the entire fundamental requirement to run a medical or dental school.
5.3. QUANTITY AND QUALITY: Number of students admitted to the medical and dental Colleges should be based on quantity and quality of teachers and teaching facilities.
5.4. FALSE HOPE: Doctors should not raise false hope of patients and their relatives that they cannot fulfill and end up disappointing them.
5.5. AVOIDING NEGLIGENCE: Doctors should avoid negligence and each patient should be adequately examined, investigated and treated.
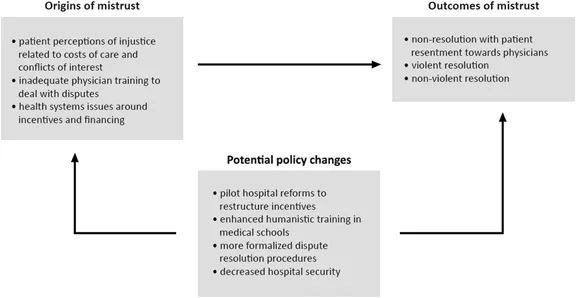
Figure 4: Origins, outcomes and policy responses of patient-physician mistrust.
5.6. EXPERIENCED PROFESSIONAL ADMINISTRATORS: Healthcare facilities should be run by experienced professional administrators, who have vast experience in diffusing a possible violence inciting scenario.
5.7. EFFICIENT SYSTEM: An efficient system should be introduced to enhance better communication between medical staff, patients and their relatives to build an atmosphere of trust among them.
5.8. CONFIDENCE BUILDING: Patients should be taken into confidence prior to any medical procedure is carried out and should be briefed about all the possible complications and risks involved in the procedure. Proper documentation should be prepared to record patient’s decision in order to prevent any misunderstanding to occur in case of failure of the medical procedure.
5.9. PERIODIC UPDATES: Patient and their relatives should be updated timely about the ongoing medical procedure so that they may know what actually is happening. Periodic updating of the condition of the patient to the attendants is necessary.
5.10. PUBLIC RELATIONS: All healthcare facilities should be made to hire professional public relations experts so that they might tackle the media and thus abstaining them from portraying a negative image of medical professionals or by asserting extra pressure on them.
5.11. PEMRA’S ROLE: Pakistan Electronic Media Regulatory Authority (PEMRA) should educate Media, in particular, to show responsibility while reporting health issues and avoid graphic details that may stir the sentiments of the people that may incite the violence.
5.12. SECURITY: Healthcare facilities should be secured with adequate security. The boundary walls of the institute should be guarded 24/7. The entry point of the hospitals should be secured by appointing physically capable security guards who should be well trained in peaceful crowd control techniques. Security guards should be posted inside the hospital particular in most sensitive areas like Emergency, Intensive Care Units, and Operation Theaters.

Figure 5: SECURITY GUARDS
5.13. BEST STAFF: Best staff should be assigned in critical areas of the hospital like Emergency wards. ICUs, Operation theaters etc. to ensure that patients needing immediate treatment get the best treatment and the chance of their survival increase.
5.14. CONSULTATION: Satisfaction of patient and their relatives regarding the ongoing medical procedure should the priority of the medical staff. The patient should be allowed to get second opinion or consultation from multiple doctors to ensure their satisfaction.
5.15. AWARENESS: Seminars and social events should be organized to educate medical professionals on how to deal with the public effectively and efficiently.
5.16. ONE GUEST POLICY: Not more than one patient’s relative should be allowed to accompany the patient to the hospital. This policy is very successful and has been adopted by many hospitals like Rehman Medical Institute (RMI) and North-West Hospital in Peshawar; which helped in mitigating the problem of overcrowding, violence etc. and keeping medical professional safe.
5.17. NO SYNDICATES POLICY: An atmosphere of harmony should be created between the senior doctors and young doctors. Recent cases of violence against senior doctors carried by young doctors organizations have created a gang war like situation in the hospitals which caused uncertain atmosphere in the hospitals where young doctor have hostile sentiments against their seniors and vice versa. Patients are the most affected party in case of conflict between the young and senior doctors rift. The government should pay heed to the demands of all parties to ensure patients don’t suffer due to internal politics of the hospitals. All political syndicates should be banned in hospitals.
5.18. HELP FROM TECHNOLOGY: Help should be sought from newer technology advancements and equipment like closed-circuit television (CCTV), and other intelligent solutions should be installed in hospitals and a team of professional especially dedicated to looking after this equipment and keeping an eye on the doctors; evaluating their performance and checking condition of the patients, while not invading their privacy while carrying on this process. CCTV can also help to track down the violators.

Figure 6: CCTV

Figure 7: CCTV MONITORING ROOM
5.19. PROTECTION FOR AMBULANCES: Even if medical professionals working inside the hospital are protected from the wrath of the patient’s relatives, but structures like ambulances can be exposed to the angry mob and can be damaged easily while also inflicting serious injuries to the ambulance staff like a driver, nurse etc. The government should be responsible to provide extra mobile security for the ambulances so that they can carry on their function uninterrupted. Special bulletproof ambulances should be provided to hospitals in order to save the staff from an armed angry mob.
 Figure 8: AN AMBULANCE SET ON FIRE
Figure 8: AN AMBULANCE SET ON FIRE
5.20. HOTLINE: A hotline should be established between hospitals and nearby Police stations so that Police can come in time when things get out of hand.
5.21. RAPID RESPONSE TEAM: A rapid response team should be raised in hospitals or nearby Police stations so that it can come to the rescue of the medical staff as soon as the turmoil begins.
5.22. INCREASED BUDGET: A significant increase in capital in the annual budget for the health sector by the Government of Pakistan can ensure that all the hospitals can have all the essential equipment that they can utilize to treat the patients. In recent years the problems like load shedding created a lot of problems for doctors, who were forced to carry on major operations using flashlights. One can imagine how a little error in such situation can affect patient. In such a scenario, the death of the patient can become justifiable for the violence carried on by the relatives, in people’s eyes.

Figure 9: DERA ISMAIL KHAN: Dutiful doctors in Dera Ismail Khan carried out a record-breaking series of 16 operations, saving lives under illumination from their cellphone torchlights.
5.23. STRICT VISITING HOURS: The patient relatives should be allowed to accompany patient for a limited time so that medical staff faces no hindrance from the relatives.
5.24. IDENTIFICATION: All the patient’s relatives or guests should be issued entry cards after complete investigation of their bio-data. This investigation record can later help the Hospital and Police administration to track down people who might be involved in act of violence carried against Hospital staff.
5.25. COMPLAINT CELL: A complaint cell should be established in every hospital to pay heed to the patient and their relative’s complaints. All the necessary actions should be carried out to satisfy them. Justice should be provided to them.
5.26. MEDICAL COST: Most of the patients or their relatives complain about how expensive the medical procedures are. This complaint gets more strength in case of death of patients; the relatives get furious as they say that they paid a large amount to cure their patients.
5.27. BLACK MARKET: Albeit being a doctor is still considered a very noble profession in Pakistani society but actions of some doctors have raised a serious question mark on this Nobel profession. Hospitals and Doctors are nowadays considered tantamount to money making machines. Private clinics run by doctors are busying in looting patients from their hard earned money both hands. Greed has intoxicated some doctors so much that they got involved with criminals and are committing some actions so unethical that violence against them in some cases seems justifiable (although it is completely condemnable). Some vice Doctors have steeped so low that they are involved in kidnapping and trafficking of newborn infants; illegal organs culture; transplantation of vital human organs from patients without their permission during operation, when they are sub-conscious and selling them to criminals, who sell them in black market; selling of used equipment like syringes etc. for cheap price. The list of such criminal activity can go on. The government should take definitive measures against the culprit to ensure justice is a server to the criminals & people can again trust the health setting authorities.
- CONCLUSION: In short, there is an urgent need to make the healthcare facilities a safe environment for the healthcare professionals to work only then they can be expected to work with devotion and dedication. Breaking News on the Television Channels regarding the death of patients due to doctor’s negligence has only served to work against the patient’s own interest as now the healthcare professionals are very reluctant to handle serious cases, hence many precious lives which could have been saved are being lost. The blind pursuit of financial profits at a systems level has eroded physician trust in Pakistan. Restructuring incentives, reforming medical education and promoting caregiving are pathways towards restoring trust. Assessing and valuing the quality of caregiving is essential for transitioning away from entrenched profit-focus models. A number of effective measures can be undertaken by the government, hospitals, and medical schools ensuring patient safety. However, it is essential to sensitize the hospital directors to elevate their quality of medical services.
- REFERENCES
1.http://pakistan.onepakistan.com.pk/news/city/301206-emergency-dept-ransacked-doctors-beaten-after-patient-dies.html - http://www.who.int/topics/violence/en/
- http://www.jem-journal.com/article/S0736-4679%2811%2900522-1/abstract
- http://www.kmuj.kmu.edu.pk/article/view/11811/pdf
- Algwaiz WM, Alghanim SA. Violence exposure among healthcare professionals in Saudi Public Hospitals. A preliminary investigation. Saudi Med J 2012;33(1):76-82.
- SOURCE: Xu D, Sun BZ, Wan XH, Ke Y. Reformation of medical education in China. Lancet 2010; 375:1502-1504.