Synopsis
In this comprehensive review, Dr. Ralph Baric emerges as a central figure in virological research, particularly concerning RNA viruses like SARS-1 and SARS-2.
His collaborations with the Wuhan Institute of Virology and his pioneering work on Zinc + Ionophores to inhibit RNA viral replication underscore his significance.
Despite Baric's critical role, there's a notable lack of recognition for his contributions, especially in the early treatment protocols utilizing Zinc + HCQ, which were sidelined in favor of more expensive treatments like Remdesivir, a drug Baric Labs created in a partnership with Gilead Sciences.
The review raises questions about the motives behind discrediting effective, low-cost treatments and the absence of further research into Zinc-based therapies, suggesting a potential disconnect between scientific evidence and treatment decisions.

Treatment
So, let's review what we've learned about Dr. Ralph Baric. Firstly, he is one of the foremost virological experts on the planet. His 40-year focus on RNA viruses is extensive and involves both SARS-1 and 2-related viral research. He collaborated with the primary researcher from the Wuhan Institute of Virology, Zhengli "Bat Lady" Shi. This includes obtaining a patent on a chimeric (clone) virus that is 80% identical to SARS-2.
Secondly, he is a member of the pre-eminent US Academy of Sciences (Microbial Biology), which has 2400 members, 190 of which are Nobel Prize winners. Pretty exclusive company which cements Baric’s reputation as an impeccable scientific viral researcher. Perhaps, it may also have been his reward for maintaining his silence and compliance related to cheap, natural, antiviral therapeutic protocols.
Thirdly, we’ve discovered that the entire foundation for EARLY Zinc + HCQ treatment protocols during the SARS-2 pandemic was inspired by the 2010 research Baric conducted on Zinc + Ionophores to inhibit RNA viral replicase (RdRP), as this writer brought to the public’s attention in late May 2020.
But as seen in the Medcram analysis, no mention of Baric’s name role is mentioned, despite many EARLY treatment protocols being created based upon that Medcram video, inspired by Baric’s “orphan” research. It deserved the title “orphan” because no record shows that such research was continued by Baric’s team, despite the incredible results it demonstrated.
We also know this was rather strange research for Baric to delve into since he used completely natural ingredients, Zinc + Pyrithione, to accomplish the inhibition of RdRP. Since the ingredients were natural, they could not be patented as a potential drug protocol, correct?
And finally, we learned that ACE2, the preferred binding receptor for the SARS 1 & 2 viruses (the only ones known to target ACE2 in humans) are Zinc-based, but lack any indications of potential ramifications due to that connection to Zinc. And lastly in our review, we have learned from the Medcram video that Chloroquine (HCQ) is a potent Zinc Ionophore.
End of Review.. Forward March!!!
I have been unable to find data that compares HCQ to Pyrithione as a Zinc Ionophore. Thus, it is currently impossible to make a comparison between the two. What we DO KNOW is that a bizarrely extensive and widespread effort was immediately undertaken to discredit the use of HCQ as a treatment for COVID, whether in the hospital or as EARLY treatment. The drug was labeled “dangerous,” despite decades of evidence for its safe and effective use against Malaria in all age ranges. This disparagement of HCQ continues to this very day, with widespread restrictions still in place in many pharmacies.
The reason I have not delved deeper into the Chloroquine story, as of yet, is that it's worthy of several articles all by itself. But I can offer some interesting facts about HCQ in 2020.
First, in all notable clinical trials, it was used ONLY on hospitalized patients, and NOT for early treatment to halt viral replication, per Baric’s based research. Furthermore, after President Donald Trump’s promotion of HCQ in March 2020, it finally obtained Emergency Use Authorization (EUA) status ONLY FOR hospitalized patients on March 28th, 2020. The law states that only one EUA can be in place for the treatment of an illness, as emergency use. And if such a drug is efficacious, then potential vaccines, such as the mRNA then being pursued, would be required to undertake the full traditional safety testing.
Thus began a flurry of immediate clinical trials on HCQ in hospitalized patients, all seemingly bent upon disproving/denouncing the its efficacy in Covid. This included the NOTORIOUS and fraudulent Surgisphere study, which was published in the previously impeccable medical journal, “The Lancet”.
LancetGate: Is Surgisphere the company that provided the data for the study serious?
From LancetGate to the certification of data on hydroxychloroquine: a look back at the scandal of the abandonment of an effective anti-Covid-19 treatment
Though beyond the scope of this article, it’s an interesting read and has bearing on The Baric Files, soon to be addressed. But here is a link to the fraud that forced The Lancet to eventually retract the paper, resulting in wide ridiculed for not having conducted a better review process before its hurried release. Difficult to find a good link that isn’t paywalled, I’ll settle for the “unbiased” (wink, wink, nudge, nudge) Wikipedia entry:
"Surgisphere is an American healthcare analytics company established in 2008 by Sapan Desai. Originally a textbook marketing company, it came under scrutiny in May 2020 after it provided large datasets of COVID-19 patients that were subsequently found to be unreliable. The questionable data were used in studies published in The Lancet and The New England Journal of Medicine in May 2020, suggesting that COVID-19 patients on hydroxychloroquine had a "significantly higher risk of death". In light of these studies, the World Health Organization decided to temporarily halt global trials of the drug hydroxychloroquine to treat COVID-19. After the studies were retracted, the WHO trials were resumed and then discontinued shortly after."
Remdesivir
What many people are unaware of is that our very own Ralph Baric is ALSO linked to the development of Remdesivir (RDV). Oddly enough, or perhaps more than coincidental, RDV is ALSO designed to target/inhibit the RNA viral RdRP Replicase, the very same target as Baric’s research on Zinc + Zinc Ionophores (including natural ones like Pyrithione).
“Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency”
Ralph Baric’s role in creating RDV.
Remdesivir, developed through a UNC-Chapel Hill partnership, proves effective against COVID-19 in NIAID human clinical trials
Ralph’s BABY!!!
On June 15, 2020, having successfully torpedoed the use of HCQ with their fraudulent and poorly designed Surgisphere and "Solidarity" studies (where hospitalized patients were often given excessive, even potentially lethal, doses of HCQ, intentionally?), the EUA for HCQ was revoked.
Oh, and by the way, one of the studies cited in that revocation was the FRAUDULENT Surgisphere study published and later retracted by The Lancet!!!
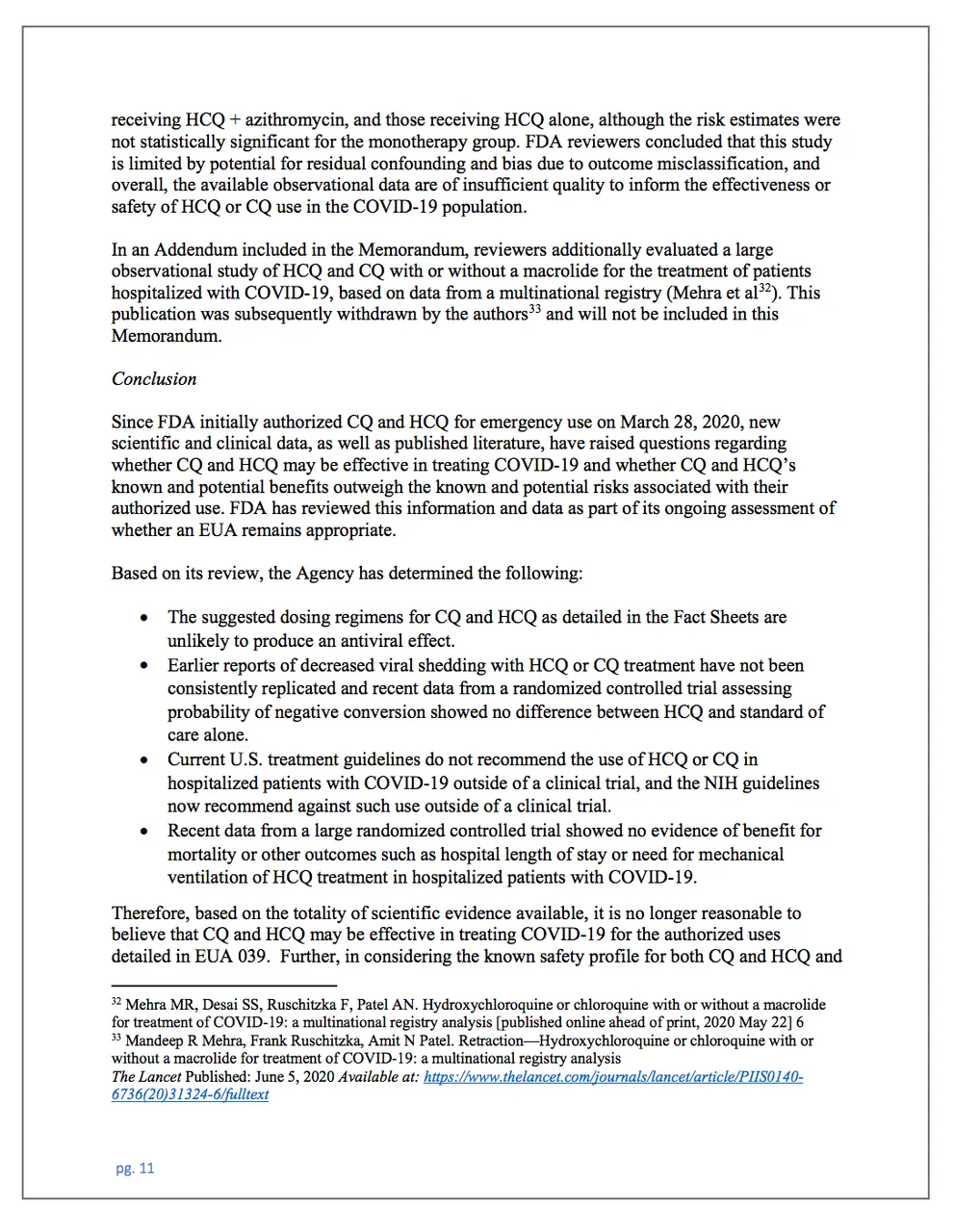
In the FDA revocation order this citation can be found at the bottom of Page 11 https://www.fda.gov/media/138945/download
What drug replaced HCQ as the new EUA offering? Well, that would be Remdesivir!!! The plot thickens, does it not? Or, perhaps just sheer coincidence?
Using RDV has an inherent problem when it comes to being used as an RdRP inhibitor. Costing upwards of a reported $3000 per treatment (versus less than $20 for Zinc + HCQ), RDV can ONLY BE ADMINISTERED VIA AN IV INFUSION, requiring patient hospitalization. That means the patient must be in a hospital bed, under a doctor’s care. And that is, simply put, TOO LATE for an antiviral drug to be effective as an RdRP inhibitor!! Treatment must be given EARLY to block the RNA viral replication, right? If you disagree, watch the Medcram video again to understand why.
So, given what we know based on Baric’s research, as analyzed by Medcram, they made a cheap and effective protocol that can be, and has been, administered in an OUTPATIENT setting and denied its use for EARLY treatment. Then they replaced it with a PATENTED $3000 drug treatment that could only be given TOO LATE to halt the RdRP viral replication effectively as patient had already transitioned into the hyper-inflammatory response (Covid) stage.
But perhaps they knew, and there was A REASON that they chose RDV, aside from the profit motive. Because it would be relatively useless as an RdRP inhibitor for hospitalized patients. And maybe even, as has been asserted in legal litigation, RDV may have serious side effects on such weakened patients that may have led to their deaths?
It begs the question: When is the IDEAL time to use an antiviral protocol? Logic and science say it MUST BE USED, either prophylactically or immediately upon presentation of an RNA viral infection (fever, etc.). So, why would a doctor WAIT for the patient’s viral loading to peak, with the patient in inflammatory immune response necessitating their hospitalization? For an oncologist treating a cancer patient, this would amount to waiting until the patient had reached Stage 4 before commencing chemotherapy, would it not? The more effective manner to treat both an RNA viral infection or cancer is to catch it EARLY and treat it EARLY with effective protocols. Ironically, Zinc sufficiency appears to play a SIGNIFICANT role in both maladies (to be addressed in an upcoming article).
Does anything I’ve written thus far violate basic logic and medical ethics?
Does it appear that there was an intentional agenda to thwart the use of EARLY treatment with RdRP inhibiting protocols, whether Zinc + HCQ, or Remdesivir?
Is it not rather interesting that Baric’s research played a direct role in both effective EARLY treatment protocols as well as the INEFFECTIVE use of RDV in hospitalized patients?
Is RDV effective? Permit me to address an interesting animal study where RDV was used on laboratory Macaques (apes) with amazing results. This study was published on June 9th, 2020, but the animal experiments were conducted in April 2020, just a few months, both just prior to Remdesivir being given EUA status on October 22nd, 2020. It very likely played a significant role in that approval.
FDA letter approving Remdesivir
In the macaque study:
Preprint version from April, 2020
See where they gave the RDV 12 hours AFTER they inoculated the Macaques with the virus?
THAT IS EARLY TREATMENT, BY GOLLY!!
And it was VERY successful in reducing viral replication, as well as the symptoms in those lab apes!! Of course, 7 days later they “sacrificed” them to examine their lungs, so we’ll never know if the animals would have suffered the alleged long-term side effects asserted in hospitalized human recipients who received RDV.
But the researchers used EARLY treatment with Remdesivir to get it approved for EUA status, where it was then administered to human patients as LATE treatment. See what they did there? They replaced one EUA drug based on the SAME EARLY treatment methodology as Zinc + HCQ, but then made sure that it would ONLY be utilized NON-effectively in hospitalized patients. Ring the register, but still not be an effective treatment in inflamed hospitalized patients. Because, by god, we cannot have EARLY treatment for an RNA virus, right?
Okay, as a final link to the HCQ and Remdesivir competition in February, 2020, it comes right from the Wuhan. While, there is no mention of Zinc being incorporated, HCQ and RDV were compared against SARS-2. Ironically, one of the names on this paper from February 4th, 2020, is Zhengli Shi, Ralph Baric’s Wuhan Collaborator!!! And granted these were “in vitro” experiments, not live animal testing. I have found no evidence of lab experiments on laboratory animals using Zinc + HCQ. I wonder why not?
“Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.”
They KNEW in Feb, 2020 that HCQ was comparable to RDV against SARS-2. Why choose expensive RDV over HCQ, the latter of which could be given EARLY as outpatient treatment. Why would they promote RDV? Was there some unmentioned rationale for wanting to deny EARLY treatment RdRP inhibiting antiviral protocols to humanity, whether Zinc + HCQ, or Remdesivir? Was it a planned failure? Is that the real agenda against HCQ.. preventing EARLY treatment options and prophylaxis?
Furthermore, why have NO animal trials been conducted based upon Ralph Baric’s 2010 Zinc + Ionophores research? Apparently, there was no such hesitation to test Remdesivir in laboratory Macaques, using EARLY treatment. The methodologies in such an experiment would be quite similar, correct? Inoculation, provide protocol, observe results. Easy Peasy
But when it comes to a CHEAP and EFFECTIVE RdRP inhibitor, apparently testing Zinc + Ionophores, whether they be HCQ, or Pyrithione, or others, such as EGCG and/or Quercetin, no one was willing to conduct such research in animals, or humans.
Something to thinking about...
I wonder why not? Is there some mysterious reason they don’t want the public to have knowledge of, or access to, low-cost RdRP inhibitors that can be taken as prophylactic prevention, or EARLY treatment?
You’ll need to be a paid subscriber to learn the secret. Sorry, but it’s worth the price of admission.
I promise.
But in the next article, let’s discuss Dr. Vladimir “Zev” Zelenko, who was THE FIRST to conduct “IN VIVO” testing in human beings of Baric’s 2010 research. He is a man, though painted as a controversial and “dangerous” by the media, who deserves his due recognition for making Baric’s research a reality, and laying the groundwork for confronting ALL RNA viral threats through cheap, natural ingredients and EARLY treatment.*
Source: Men In Black
Previously on Men In Black
Beneficial effects of HCQ and Zinc against COVID-19
The article saying Zinc is effective against coronavirus is written by Ralph Baric in 2010.
Baric's Zinc Revelation: Part 1
Baric's Zinc Revelation: Part 2
Baric's Remdisivir Revelation: Part 3
Baric's "Zelenko" Protocol: Pt 4
HCQ and Zinc's Secrets | Baric Files Pt. 5
Epilogue(?): The Baric Files.