When Coronavirus first arrived in widespread media coverage around March 2020, the means to determining whether someone had the virus was iffy. The virus being so NOVEL, and the origination being in a country whose rulers have not been all that great with honesty and transparency, made determining how the virus would be detected a bit difficult.
And while there is a whole discourse to be had about how the original Sars-2 virus was modeled for genetic location, the focus of this article is to explain how the reporting and testing methods grossly skewed the picture.
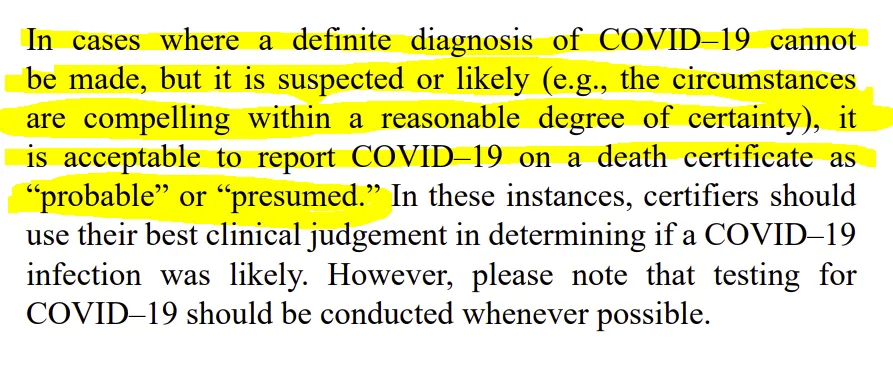
The first major distortion came when the CDC stated in their Vital Statistics Reporting Guidance No. 3 ▪ April 2020 that doctors could use a label of “probable” or “presumed” in associating Coronavirus with a death. Which meant that doctors could essentially assume that Coronavirus was the chief cause of death if they so perceived.
Link here: https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.pdf
Now you might be saying to yourself that doctors wouldn’t just label a death that way without reason, right?
They wouldn’t just willy-nilly pump the Coronavirus death numbers up out of nowhere?
Well, you’re right.
Not out of nowhere.
But out of a need to stay afloat because the government stopped elective care.
With doctors not being able to take elective appointments and people being generally more afraid to go out, cash flow was starting to run dry.
But then, the government gave doctors the best reason to go with the Coronavirus label, no matter if it was the flu or some other combination of pre-existing conditions.
The government gave out financial incentives to doctors for Coronavirus hospitalizations and placement into ICUs, with bonus funding for ventilators.
You can read more about that here:
Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators
https://www.usatoday.com/story/news/factcheck/2020/04/24/fact-check-medicare-hospitals-paid-more-covid-19-patients-coronavirus/3000638001/
(And to cut to the cliff-notes version because it’s so crucial: “We rate the claim that hospitals get paid more if patients are listed as COVID-19 and on ventilators as TRUE.”)
So now, you have a huge market distortion where the government is holding the carrot-and-stick to allow doctors to presume Coronavirus as proximate causation for death AND the ability to get more government money for labelling a patient a such.
Do you see how this could be so tempting, especially in light of denied income from elective surgeries and the murkiness of what Coronavirus symptoms could be?
(For more on the elective surgery situation, read:
Preserving Elective Surgeries in the COVID-19 Pandemic and the Future
https://jamanetwork.com/journals/jama/fullarticle/2771580 )
BUT WAIT!
There’s more.
Now that we have this incentives backdrop, the CDC made it much more easy to get that positive result “legitimately” (on the “books”) by recommending the use of PCR tests.
For those of you not familiar, according to the Cleveland Clinic “the polymerase chain reaction (PCR) test is performed to detect genetic material from a specific organism, such as a virus.”
See: https://my.clevelandclinic.org/health/diagnostics/21462-covid-19-and-pcr-testing
In layman’s terms, the virus’ DNA is broken apart into two strands (denatured) using heat, and then the remaining two strands are recombined with a primer (something that combines with the DNA to match and make it whole again), causing a duplication of the DNA genetic material. This process is repeated until you have an exponentially larger amount of that DNA, so much so, you can observe what someone may have.
You can get a little more in-depth on the topic by watching this video if you wish: 
There’s just one catch: the more you do this process, the more room there is for error after a certain number of cycles.
The errors can come in the form of amplifying the wrong virus OR amplifying a virus that really isn’t at a sufficiently high enough load to be contagious in a person. i.e. There may be a small bit of a specific viral DNA in the person, but not enough to be sick/contagious.
So, at what threshold do these errors become more problematic? Most PCR specialists agree that 35 cycles and higher is where the data becomes VERY problematic.
Even Dr. Fauci agrees with this, as you can see here:

Kary Mullis, the inventor of PCR and winner of the Nobel Prize for that accomplishment, also noted the issues with both PCR testing AND Dr. Fauci long before Sars-2 was a thing.
You can watch that here:
Kary B. Mullis – Interview on Fauci

What Kary Mullis says about PCR testing

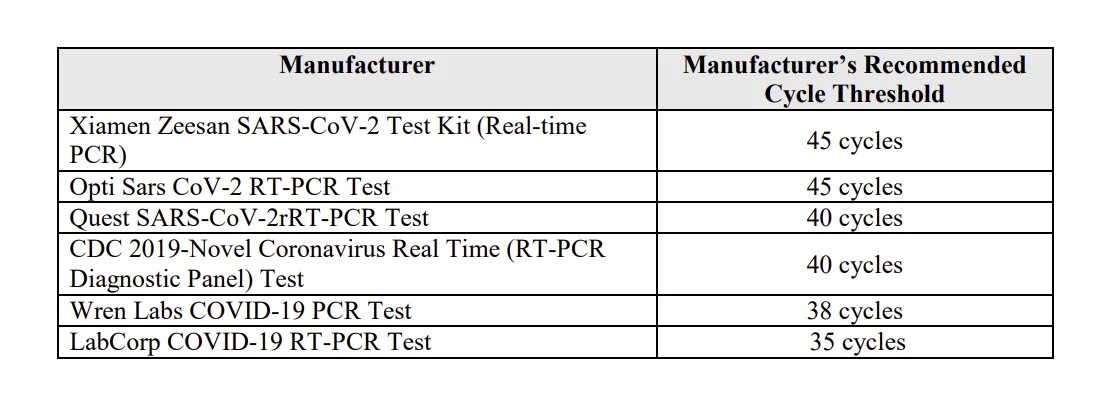
So now that we know that 35+ cycles can lead to some unreliable data, what cycles were labs using for PCR tests?
Well- funny thing, the CDC never required labs to report what cycles they’re using.
BUT, from what is known in some independent research as in an injunction filed by America’s Fontline Doctors, it appears that the cycle rates have been quite high across many labs.
See:
Full injunction: https://www.scribd.com/document/516493624/Motion-for-Preliminary-Injunction-File-Stamped
And this oddity has lead to some intriguing outcomes, such as a man who died in a motorcycle crash being counted as a “Coronavirus Death” because he tested positive.
See:
Man who died in motorcycle crash counted as COVID-19 death in Florida: Report
https://wpde.com/news/nation-world/man-who-died-in-motorcycle-crash-counted-as-covid-19-death-in-florida-report-07-18-2020
On top of that, the CDC reported that 94% of those labelled with Coronavirus death have 2.6 comorbidities.
See:
News: 94% of patients who died from COVID-19 had complicating conditions, data confusion surrounding virus risk
In raw terms, that means that there is a trend toward having 3 more conditions as 2.6 is above the half-way mark between 2 and 3, and no one has “half a condition.”
Some try to downplay this as just being benign issues with the elderly, such as weak bones or a cold.
But if you look at the CDC's data here:
https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm
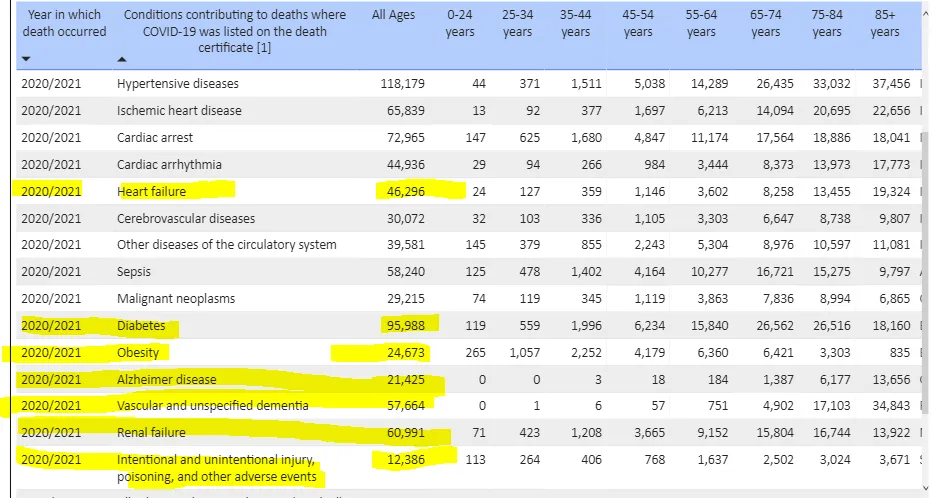
There are over 100,000 independently-deadly comorbidity cases listed, including things like accidental injury.
It’s not just someone having a rash or the sniffles.
So where does this leave the CDC data as to death counts?
It leaves it largely in a black box.
The reality is that we don’t know for sure how many people died chiefly because of Coronavirus symptoms.
But what we do know is that:
1.) The government opened the door to make labelling Coronavirus deaths easy.
2.) The government offered a financial incentive to doctors to use the Coronavirus death label.
3.) Doctors had a motive to do so because they were losing money with a lack of patients.
4.) PCR tests gave labs and doctors the perfect way to get to a positive result using an independent instrument, as no matter how little or non-present ACTUAL Sars-2 genetic material there was in a patient, with enough cycles, one could get to a case.
Scary, huh?
#coronavirus #covid19 #corona #sars2 #vaccine #vaccines #coronatruth #endthelockdown #endtheshutdowns #endthelockdowns #endtheshutdown