Hello steemians, last week I wrote about myelodysplastic syndrome but I didn't go deeper. It's was kind of an introduction and a general knowledge about it's clinical significance. Today's edition of my blog will seek to help medical laboratory personells as well as physicians to understand and know the FAB system of classifying MDS. Without much I do, let's get started!!!
The French-American-British (FAB) group in 1982 classified myelodysplastic syndromes according to morphology of cells and the proportion of myeloblasts after a bone marrow smear and peripheral blood smear examination.
From the above basis, MDS can be classified as;
In RA, the proportion of myeloblasts is less than 5% in bone marrow and also less than 1% of total nucleated cells in peripheral blood. RA has little or no chance of transforming into acute myelogenous leukemia (10-20% chance). Usually, the bone marrow is hypercellular which is associated with erythroid hyperplasia. There is also the incidence of thrombocytopenia with larger granular platelets, reticulocytopenia with dysplasia in only the erythroid series and basophilic stippling of red cells. Ringed sideroblasts observed but is less 15% in bone marrow. NOTE that in RA, granulocytic and megakaryocytic series appear normal.
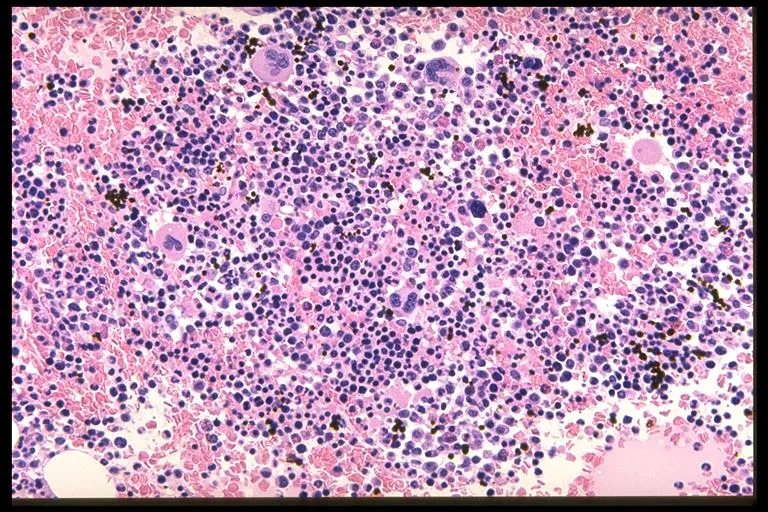
Source
RARS is characterized by the proportion of myeloblasts being less than 5% of total nucleated cells in bone marrow and also less than 1% in peripheral blood. The distinguishing feature of RARS is the presence of ringed sideroblasts which exceeds 15% of total erythroblasts. Neutopenia, thrombocytopenia and trilineage dysplasia is less common in RARS than in RA. In addition, RARS sometimes comes with two blood cell populations - a major normochromic macrocytes and a minor population of hypochromic microcytes.
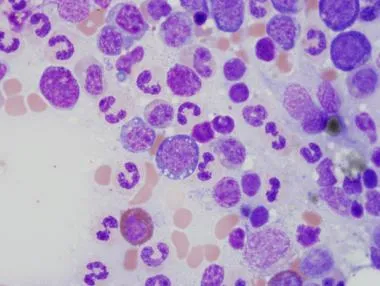
Source
In RAEB, the proportion of myeloblasts is equal to or greater than 5% and can comprise up to 20% of total nucleated cells. In the peripheral blood, the blast cell count is less than 5%. RAEB is more likely to transform into AML. In contrast to refractory anaemia, dysgranulopoiesis is a common feature and trilineage dysplasia is more severe under this category ofMDS than in RA. Bone marrow examination reveals a hypercellular bone marrow with variable degree of granulocyte or erythroid hyperplasia.
Similar to RAEB, this condition is distinguished by any of the following:
People with CMML may have shortages of some blood cells, but a main problem is too many monocytes. Often, the monocyte count is much higher, causing their total white blood cell count to become very high as well.
Usually there are some abnormal cells, called blasts, in the bone marrow. The amount of blasts in CMML is below 20%. In the peripheral blood, the blast cells are less than 5% of total nucleated cells. Many people with CMML have enlarged spleens. About 15% to 30% of people with CMML go on to develop acute myeloid leukemia.
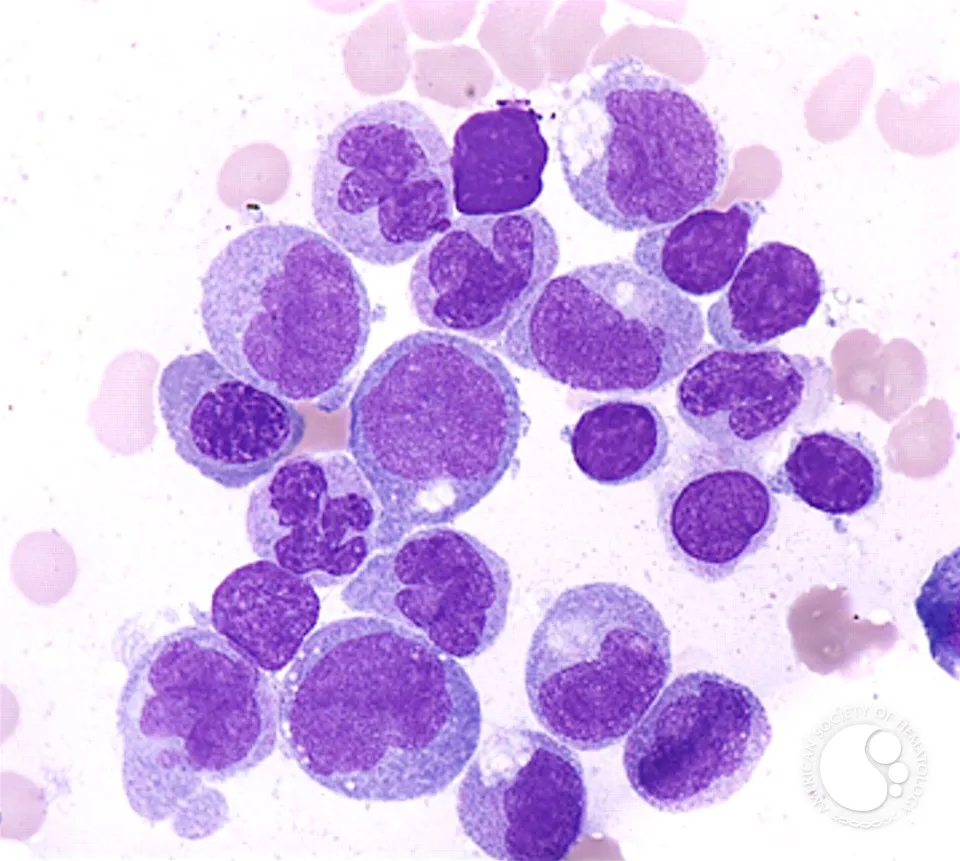
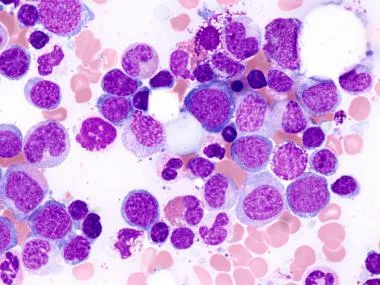
This is an image showing dysplastic promonocytes. CMML is mostly characterised by a hypercellular BM with dysplatic promonocytes.